
Welcome to Health Policy Institute
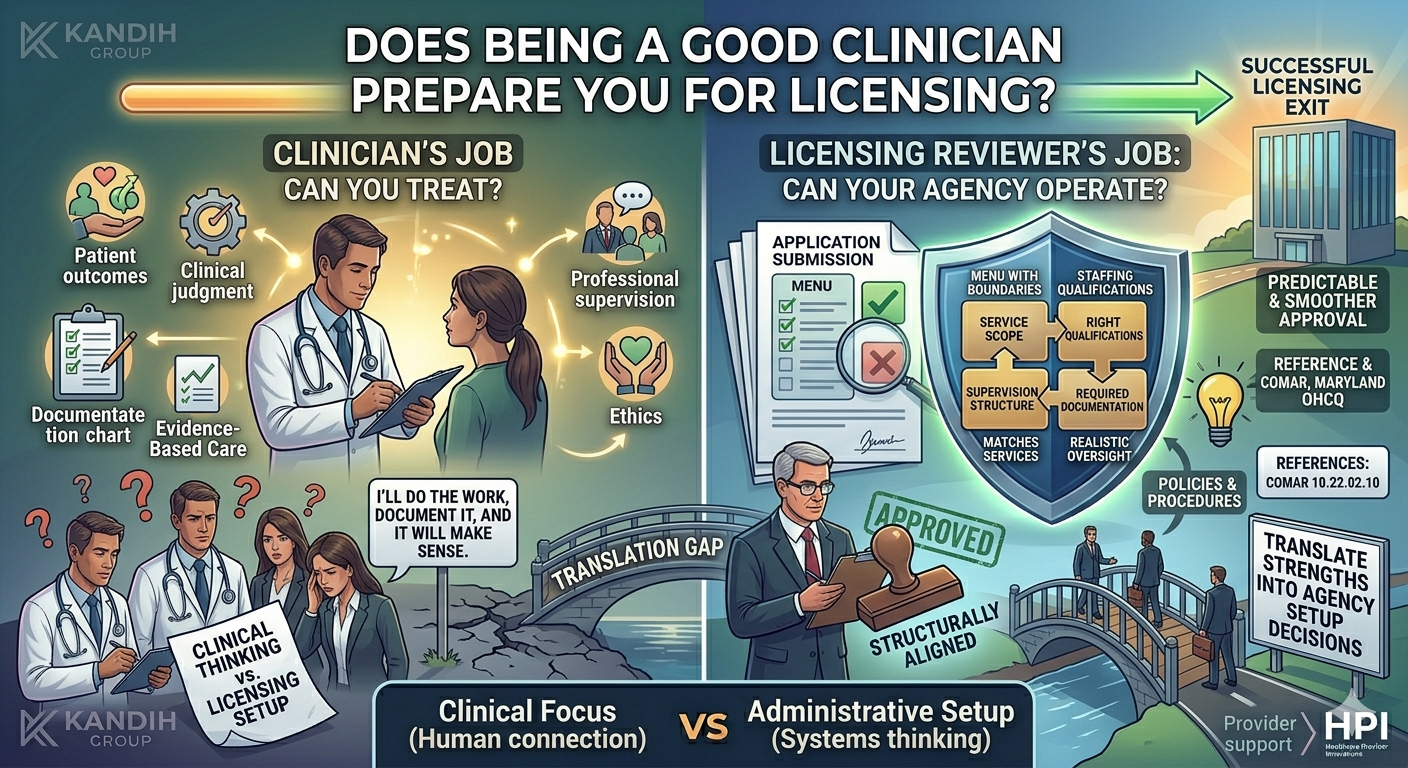
A clinician-owner once said, “I know how to treat patients. I know how to lead a team. Why does licensing feel like I’m starting from zero?” Because licensing isn’t testing your clinical ability. It’s testing whether your agency is set up to operate under a specific license pathway—with a clear service scope, the right staffing qualifications, a workable supervision structure, and required documentation that matches the services you’re applying to provide. Being a great clinician helps. But it doesn’t automatically prepare you for licensing. Clinical skill and licensing are two different jobs Clinical skill answers: “Can you treat?” As a clinician, your work focuses on:
patient outcomes clinical judgment documentation in the chart evidence-based care professional supervision and ethics That’s the world you’re trained in. Administrative setup answers: “Can your agency operate?” Licensing focuses on the agency as a system: What services will you provide (service scope)? Who is qualified to provide them (staffing qualifications)? Who supervises the work (supervision structure)? What policies and required documentation prove the agency can deliver the service model? A reviewer can’t approve “this clinician is talented.” They approve a structure that matches the license category.
Why clinicians feel blindsided by licensing Clinicians often approach licensing the same way they approach patient care: “I’ll do the work, document it, and it will make sense.” Licensing doesn’t work that way. Licensing is more like building a clinic on paper before it opens. If your setup decisions are unclear, the application submission can be returned or delayed—even if the forms are filled out perfectly. The most common gap: service scope vs clinical thinking Clinicians naturally describe services like clinical work: assessments treatment planning progress notes discharge Licensing wants something different: a clear service scope with boundaries. Example founders recognize: You describe “support services,” but the description includes clinical treatment tasks. Now the reviewer can’t tell which license pathway fits, because the service scope reads like two models at once. The second gap: staffing qualifications vs “we’ll staff it later” In clinical practice, you can often adjust staffing as you grow. In licensing, staffing qualifications must match the services described at the time of application submission.
Example founders recognize: “We’ll hire the qualified supervisor after approval.” If the service scope requires that oversight, the reviewer usually pauses because the model isn’t supported yet. The third gap: supervision structure vs informal supervision Clinicians are used to supervision being part of team culture: consults, case review, peer support. Licensing requires supervision structure to be clearly defined: who supervises whom what oversight looks like who is accountable for decisions If this is vague, reviewers slow down because accountability isn’t clear. The fourth gap: policies vs clinical standards Clinicians often assume, “Policies are just standard templates.” But licensing reviewers compare policies to your service scope and staffing model. If policies mention services you don’t provide or roles you don’t have, it signals misalignment. Some provider frameworks explicitly require agencies to develop and adopt written policies and procedures, which is why generic policies can cause delays. (law.cornell.edu )
What DOES translate well from clinician to administrator Clinicians are not starting from scratch. You already have strengths that matter in licensing setup: You understand risk and accountability You respect documentation and consistency You know why supervision matters You can design workflows that protect clients The shift is learning to translate those strengths into agency setup decisions. A simple way to know you’ve switched into “administrator mode” You’re thinking like an administrator when you can answer these clearly: What is our service scope (and what are we not offering)? Do staffing qualifications match that scope? Is supervision structure clear and realistic? Do policies match the exact services we’re applying to provide? Does the application submission tell one consistent story? When those answers are clear, licensing becomes easier. Where HPI comes in (setup only) This is exactly where clinician-owners benefit from support—before submitting. HPI helps clinicians shift from “clinical thinking” to “licensing setup thinking” by helping you: choose the correct licensing / accreditation pathway define service scope with clear boundaries align staffing qualifications and supervision structure align required documentation (policies) to the real operating model That prevents returned or delayed application submissions caused by mismatched setup decisions. Bottom line Being a good clinician is a strong foundation for running a healthcare agency. But licensing requires a second skill set: administrative setup—service scope, staffing qualifications, supervision structure, and required documentation aligned to the right pathway. Once you treat licensing as agency design (not paperwork), it becomes far more predictable.