
Welcome to Health Policy Institute
A founder once told me, “I just want to know who to apply to first.” Fair question. It sounds like there should be one clean answer. But here’s what usually happens: you pick a regulator, start filling out an application submission, and then someone says, “Wait—your services actually fall under a different pathway.” Now you’re rewriting your service scope, fixing staffing qualifications, rebuilding your supervision structure, and trying to make your required documentation match a new direction. That’s why application order depends on what services you’re offering, not what type of business you think you are. The core idea: licensing order follows your service scope Before you decide who to apply to first, lock one decision: What services will you actually provide in the first 6–12 months? That is your service scope. Regulators don’t license “agencies.” They license service models. Once your service scope is clear, the correct licensing / accreditation pathway becomes much easier to identify—and the approval timeline becomes more predictable.
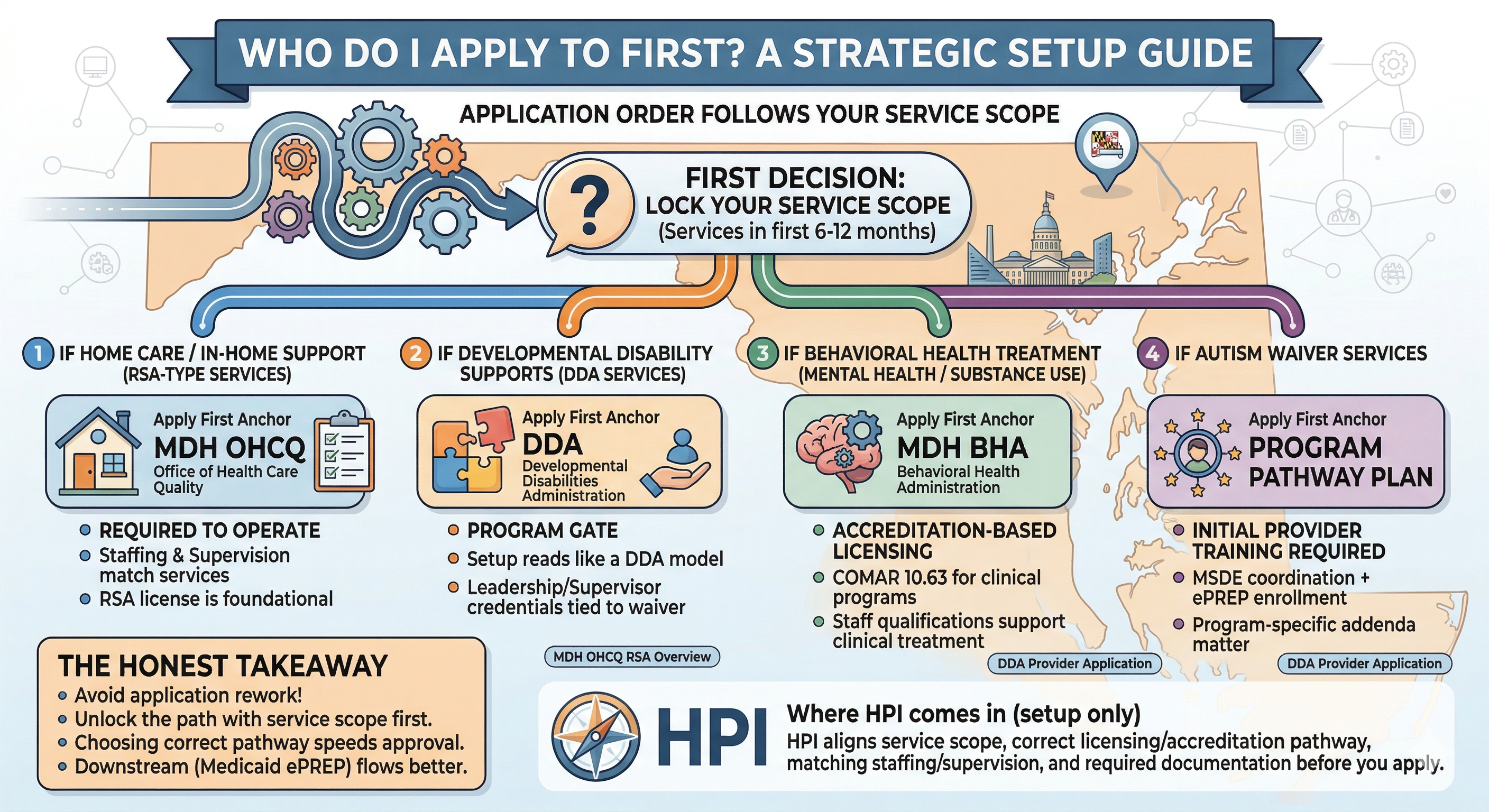
Why “application order” changes from agency to agency Some agencies only need one regulator to approve a license. Others need multiple approvals because they’re touching different systems: MDH (Maryland Department of Health) licensing (often through specific offices like OHCQ or BHA) DDA provider approval for developmental disability services MSDE involvement for Autism Waiver provider readiness/training Medicaid enrollment to get paid (ePREP) Those are not duplicates. They are different layers: permission to operate, program participation, and payment. The simplest way to choose the right “apply first” path Use this plain-language guide. It’s intentionally high-level—this is about planning, not a step-by-step checklist. If your services are home care / in-home support (RSA-type services)
Your “apply first” anchor is usually MDH OHCQ because you cannot operate an RSA in Maryland without a license from OHCQ. The RSA application instructions state you may not conduct or operate an RSA without first obtaining the license and complying with COMAR 10.07.05. If your service scope is RSA, you start there—because everything else builds on that operating authority. What to plan for: Your staffing qualifications and supervision structure must match the services you describe. If you apply as RSA but describe a different service model, you risk a returned or delayed application. If your services are developmental disability supports (DDA services) Your “apply first” anchor is usually DDA because DDA is the program gate for DDA service models. DDA also points providers to the regulatory framework that applies to DDA providers, and the provider application expects evidence of leadership/supervisor qualifications tied to waiver services. What to plan for: DDA setup is not “home care with a new label.” Your service scope, staffing qualifications, supervision structure, and required documentation need to read like a DDA provider model, not an RSA model. If your services are behavioral health treatment (mental health / substance use programs)
Your “apply first” anchor is usually MDH BHA because BHA issues licenses under COMAR 10.63 for community-based behavioral health programs and services, including accreditation-based licensing pathways for certain program categories. What to plan for: Behavioral health reviewers look closely at whether your staffing qualifications and supervision structure support clinical treatment services. If your service scope is clinical but your staffing plan reads like a support-services agency, approval slows fast. If your services are Autism Waiver services This is the one that trips people up—because it often feels like “multiple applications.” Your “apply first” anchor is your program pathway plan, not a single regulator. In Maryland, the Autism Waiver provider addendum explicitly states prospective applicants must attend the Autism Waiver Initial Provider Training and Information Session before submitting an application. Medicaid enrollment is done through ePREP, and Autism Waiver uses program-specific addenda. What to plan for: Autism Waiver involves coordination across systems (MSDE/program readiness + Medicaid enrollment requirements). If you treat it like a single license form, you end up reworking your setup. The biggest mistake: choosing order based on what you want to be.
Founders often say things like: “I’m starting a DDA agency” (but their service scope reads like home care) “I’m starting a behavioral health agency” (but they’re really offering supportive services) “I’m doing Autism Waiver” (but they haven’t aligned staffing qualifications or supervision structure to the actual waiver service model) When your service scope and staffing model don’t match the pathway, the application submission gets returned or delayed—then everything downstream (including Medicaid enrollment) moves later. A reassuring takeaway If you’re unsure who to apply to first, that usually means your setup decisions aren’t finalized yet—and that’s normal. The fix isn’t “guess and submit.” The fix is to lock your service scope first, then choose the correct licensing / accreditation pathway. That’s how you avoid false starts and protect your approval timeline. Where HPI comes in (setup only) This is exactly the pre-application point where HPI helps. HPI helps you decide the right application order by aligning: the service scope you will actually deliver the correct licensing / accreditation pathway (MDH/OHCQ, DDA, BHA, Autism Waiver program requirements) staffing qualifications and supervision structure that match that scope required documentation that supports what you’re applying to provide When those are aligned, the “who do I apply to first?” question becomes straightforward—and your application submission is far less likely to be returned or delayed.
References
- Maryland OHCQ RSA Overview (how to apply for initial RSA license): https://health.maryland.gov/ohcq/Pages/Residential-Service-Agencies.aspx
- Maryland OHCQ — Application for a Residential Service Agency License (states RSA cannot operate without OHCQ license; COMAR 10.07.05): https://health.maryland.gov/ohcq/Documents/Providers/RSA/Forms/Application-for-Residential-Service-Agency-License.pdf
- Maryland DDA Regulations Page (provider regulatory framework): https://health.maryland.gov/dda/Pages/Regulations.aspx
- Maryland DDA Provider Application (evidence of leadership/supervisor qualifications for waiver services): https://health.maryland.gov/dda/Documents/DDA%20Provider%20Application%20-%20Revised%2008-11-23.pdf
- MDH BHA — Accreditation Based Licensing (COMAR 10.63 accreditation-based licenses): https://health.maryland.gov/bha/pages/accreditation-information.aspx
- COMAR 10.63 Online Application Guide (BHA licensing under COMAR 10.63; licensing categories): https://health.maryland.gov/bha/Documents/COMAR%2010.63%20Online%20Application%20Guide.pdf
- Maryland Medicaid Provider Enrollment (ePREP Enrollment Requirement): https://health.maryland.gov/mmcp/provider/Pages/enrollment.aspx
- Maryland Medicaid ePREP Provider Agreement and Application Addenda (program-specific addenda list): https://health.maryland.gov/mmcp/provider/Pages/eprepforms.aspx
- Autism Waiver ePREP Addendum (states initial provider training required before submitting application): https://health.maryland.gov/mmcp/provider/Documents/application-addenda/40_AutismWaiver_ePREPAddendum_V1.pdf