
Welcome to Health Policy Institute
You spent years learning your craft. Nursing school. Therapy programs. Social work certifications. DDA direct support training. You know how to assess a client, build a care plan, document a session, and respond when something goes wrong. You are good at what you do — and that's exactly why you decided to open your own agency. But somewhere between that decision and the moment you sat down to fill out your first licensing form, something shifted. Suddenly the work you trained for isn't the work in front of you. Instead of care plans, you're reading regulatory code. Instead of client notes, you're writing policies. Instead of supervising staff, you're trying to figure out what an operating agreement is and why the state needs three versions of it. You're not struggling because you're not smart enough. You're struggling because the skills that make you an excellent clinician have almost nothing to do with the skills required to license a business. And nobody told you that before you started. Shape Two Completely Different Skill Sets Clinical training prepares you for one world. Business setup lives in another. In your clinical career, the system supported you. There was a supervisor. There was a compliance team. There was an administrator who handled the paperwork side while you focused on care. The regulatory burden existed — but someone else carried it. When you open your own agency, you become that someone else. Overnight, you are the clinician, the administrator, the compliance officer, and the person responsible for making sure the application meets the state's requirements before it goes in. That transition catches almost every clinician-founder off guard. Not because they aren't capable — but because the knowledge needed to navigate Maryland's RSA, DDA, or Behavioral Health licensing process isn't taught in any clinical program. It isn't covered in your licensure exam. It isn't mentioned in your continuing education requirements. It exists in regulatory documents, agency guidelines, and the institutional knowledge of people who have done this before. And if you don't have access to that knowledge, the licensing process feels like being dropped into a foreign country with no map and no translator.
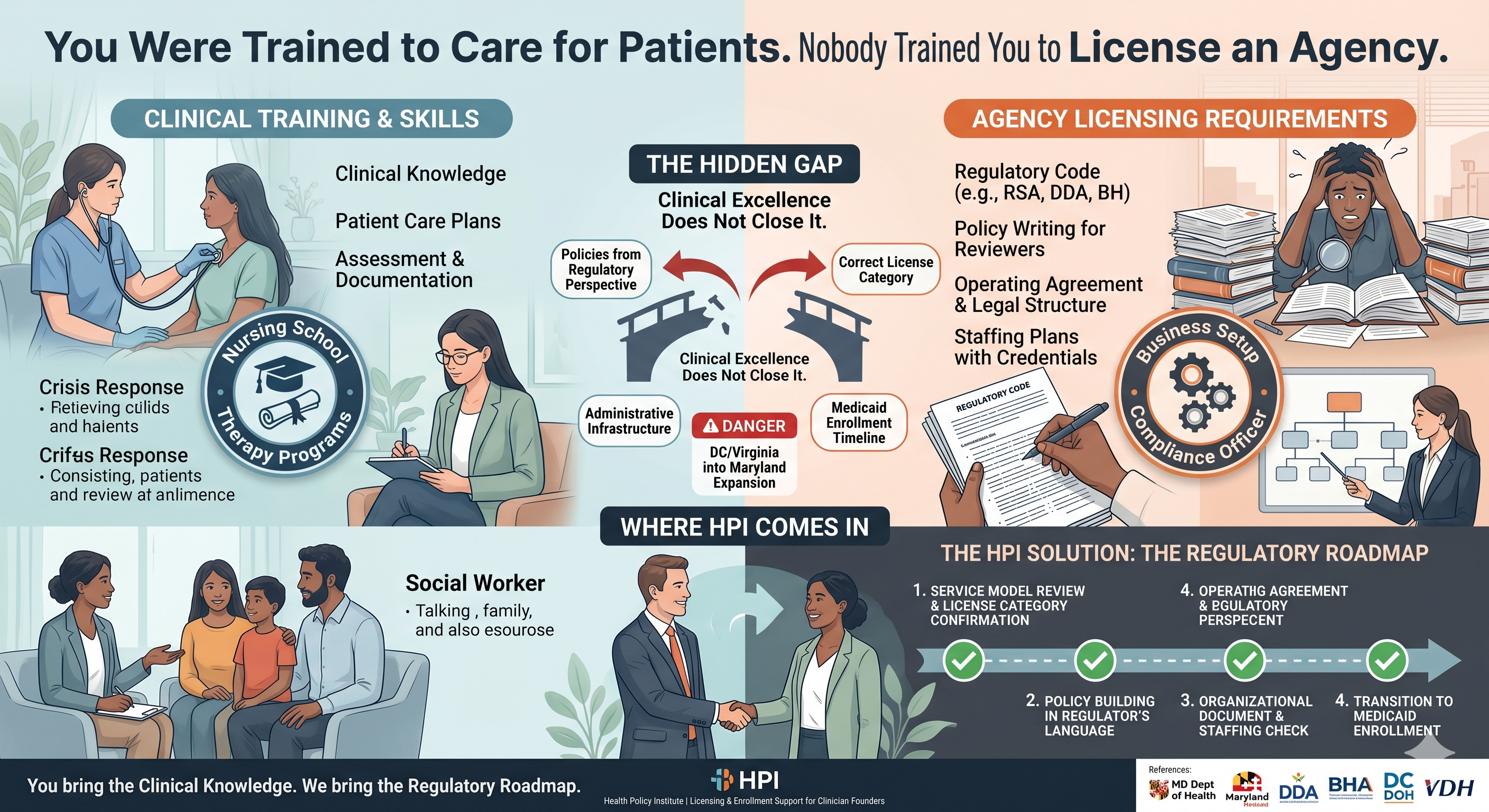
Where Clinicians Get Stuck Most Often The gaps between clinical training and licensing requirements show up in very specific places. These are the ones we see most often with clinician-founders in Maryland, DC, and Virginia. Policies written from a clinical perspective instead of a regulatory one. As a clinician, you know how care should be delivered. So when you write your policies, you write them the way you would document care — focused on the client, focused on the service, focused on the outcome. What you don't know — yet — is that Maryland reviewers are reading your policies to confirm that your agency's internal structure meets specific regulatory standards. The clinical detail doesn't help you if the regulatory language isn't there. Policies that read like clinical protocols fail review, even when the care they describe is excellent. Choosing the wrong license for your services. Clinicians working in the DDA space, the RSA space, or the behavioral health space often have deep expertise in the services they plan to offer — but limited familiarity with which license category actually covers those services in Maryland. The line between an RSA license and a DDA Supported Living license, for example, isn't always obvious until you've read the regulatory definitions carefully. Choosing the wrong one means building an entire application on the wrong foundation. Underestimating the administrative infrastructure. Your license application isn't just about what services you offer. It's about how your agency is built. Organizational documents, staffing plans with documented credentials, a physical location that meets requirements, and an administrative structure that shows the state your agency can actually function as a business — not just deliver care. Clinicians frequently underbuild this side because it wasn't part of their professional training. Medicaid enrollment coming as a surprise. Many clinician-founders don't realize until after they're licensed that Medicaid enrollment is a completely separate process with its own requirements and its own timeline. They assumed licensing meant billing. It doesn't. Finding this out after the license is issued — when the agency is already operational and overhead is running — delays revenue in ways that can seriously strain the business.
Doing it alone because asking for help feels like admitting failure. This is the quietest version of the problem. Clinicians are trained to be competent. Asking for help in a clinical setting means something is wrong. That mindset transfers into the business setup process — and it keeps founders stuck longer than they need to be, working through problems they don't have the background to solve efficiently, when someone who does could resolve them quickly. Shape What the Licensing Process Actually Demands Here's a plain-language summary of what Maryland's licensing process is actually asking you to demonstrate — not as a clinician, but as a business operator. It wants to see that your agency has a legal structure that matches your application. That your policies reflect the specific standards of your license category — written in the language regulators use, not the language clinicians use. That you have qualified, confirmed staff in the right roles with the right credentials documented. That your physical location meets the requirements for the license you're applying for. And that your entire application tells one consistent story from the first form to the last attachment. None of this has anything to do with whether you're a good clinician. It has everything to do with whether your agency is built correctly as a regulated business. That's the gap. Clinical excellence doesn't close it. Business and regulatory knowledge does. Shape The DC and Virginia Layer If you're based in DC or Virginia and looking to operate or expand into Maryland, the gap gets wider. Each jurisdiction has its own licensing structure, its own regulatory body, and its own Medicaid enrollment process. What works in Virginia doesn't automatically translate to Maryland. DDA services in Maryland operate under a different framework than developmental disability services in DC or Virginia. The terminology overlaps but the requirements don't always match. Clinician-founders who have successfully navigated licensing in one state often come into Maryland expecting a similar process — and run into requirements they didn't see coming. The framework is different. The language is different. The sequence is different. That doesn't make it impossible. It makes it something you need to learn before you assume you already know it.
Where HPI Comes In The Health Policy Institute works with clinician-founders at exactly this intersection — deep clinical expertise, limited regulatory experience, and a licensing process that requires both. We speak both languages. We understand the care side well enough to help translate it into the policy and documentation language the state needs to see. And we know Maryland's RSA, DDA, and Behavioral Health licensing requirements well enough to build an application that's correct from the start. For clinician-founders in DC and Virginia looking to expand into Maryland, we provide the Maryland-specific regulatory knowledge that doesn't transfer automatically from other jurisdictions — covering the DDA framework, RSA licensing requirements, and Maryland Medicaid enrollment from the ground up. What this looks like in practice: we review your service model and help confirm the right license category. We review or help build your policies in the language regulators are looking for. We check your organizational documents, your staffing plan, and your physical site setup. And we stay with you through Medicaid enrollment so the transition from licensed to billing is as short as possible. You bring the clinical knowledge. We bring the regulatory roadmap.
The Bottom Line Why is licensing hard for clinicians? Because licensing isn't a clinical skill. It's a regulatory and business skill — and clinical training doesn't cover it. The policies, the organizational structure, the administrative documentation, the Medicaid enrollment sequence — none of it is in the curriculum, no matter how good your clinical education was. The founders who move through this process smoothly aren't the ones with the most clinical experience. They're the ones who recognized the gap early and got the right support to fill it. Your clinical training is your foundation. HPI helps you build the rest.
References
- Maryland Department of Health – Office of Health Care Quality (OHCQ)
- Maryland Developmental Disabilities Administration (DDA) – Provider Enrollment
- Maryland Behavioral Health Administration (BHA) – Licensing and Certification
- Maryland Medicaid Provider Enrollment Portal
- DC Department of Health – Healthcare Facility Regulation
- Virginia Department of Health – Office of Licensure and Certification
- Health Policy Institute – Licensing and Enrollment Support for Clinician-Founders