
Welcome to Health Policy Institute
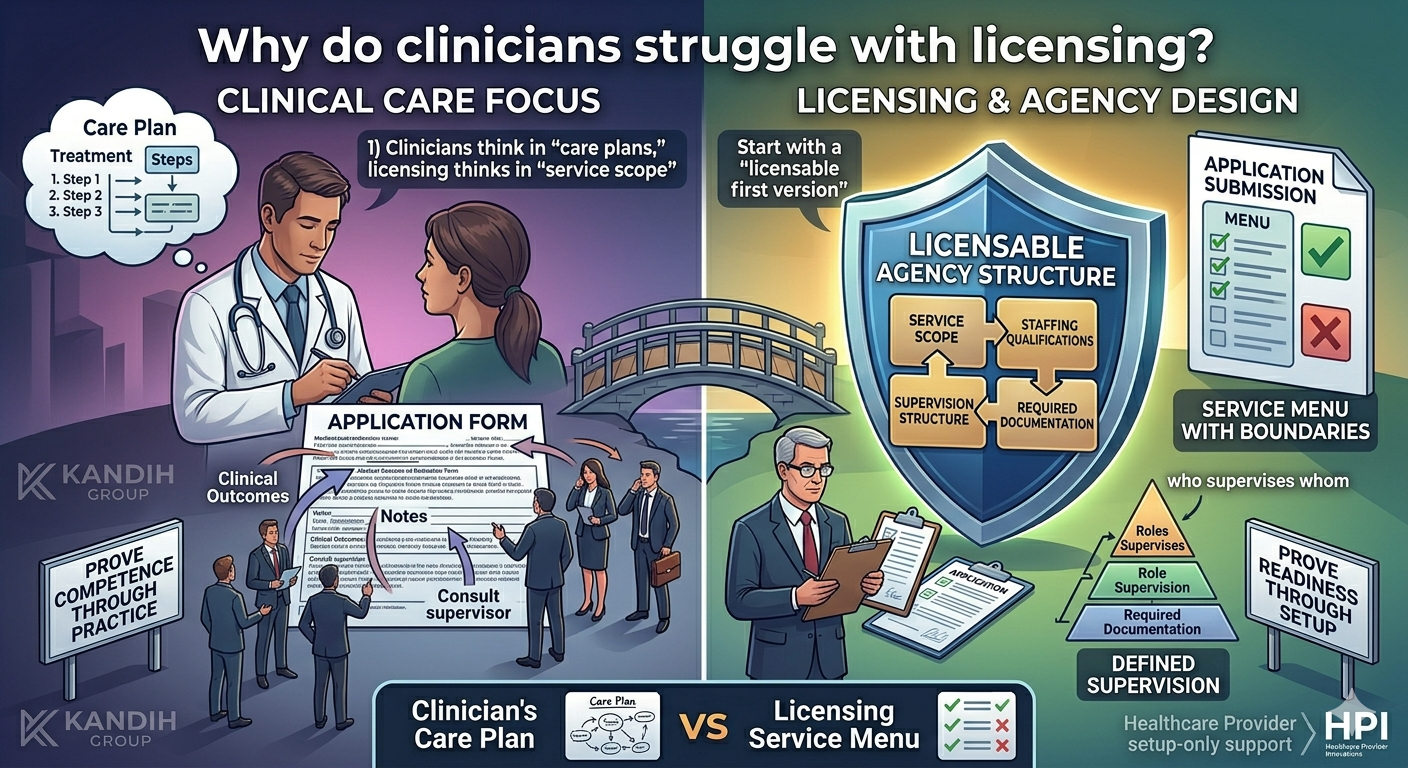
A clinician-owner told me, “I’ve treated patients for ten years. I can run a program. Why does licensing feel like a different language?” Because it is. Clinical work is built around the patient in front of you. Licensing is built around the system behind the patient: service scope, staffing qualifications, supervision structure, and required documentation—all matched to a specific licensing / accreditation pathway. Clinicians don’t struggle because they aren’t capable. They struggle because licensing asks a different kind of thinking. Licensing is not clinical practice — it’s agency design In clinical practice, you prove competence through outcomes, notes, supervision, and experience. In licensing, you prove readiness through setup decisions: What services will the agency provide (service scope)? Who is qualified to provide them (staffing qualifications)? Who supervises the work (supervision structure)? What policies and required documentation show you can operate as described?
A licensing reviewer can’t approve “this clinician is excellent.” They can only approve what the application submission proves. That’s why licensing can feel frustrating to clinicians: you’re used to showing competence through practice, not through structure. 5 reasons licensing feels harder for clinicians (and what to do about it) 1) Clinicians think in “care plans,” licensing thinks in “service scope” Clinicians naturally describe care in clinical terms: assessment, treatment planning, progress, discharge. Licensing needs you to describe services in defined categories and boundaries: what you will and will not provide.
Founder example: “I’m offering supportive services” — but the description includes clinical treatment tasks. That mismatch can lead to a returned or delayed application because the service scope doesn’t match the license type. Practical shift: Write services like a menu with boundaries, not like a treatment note. 2) Clinicians assume “competence” can fill gaps — licensing does not In clinical settings, you can sometimes adjust quickly: consult a supervisor, change staffing, update workflows. Licensing reviewers don’t assume you’ll fix it later. They approve what is clearly supported now. Founder example: “We’ll hire the qualified supervisor after we’re approved.” If the service scope requires that role, reviewers often pause because the setup is incomplete. Practical shift: Don’t rely on “later” for roles that make the model work. 3) Clinicians often underestimate how much supervision structure matters Clinicians are used to supervision being part of culture: case consults, team meetings, chart review. Licensing expects supervision to be defined as a structure: who supervises whom what oversight looks like where accountability sits If that’s vague, the reviewer can’t confirm how the agency will operate
Practical shift: Treat supervision structure like the backbone of your agency, not an HR detail. 4) Clinicians often use policy templates like “standard of care” — but licensing sees mismatch Clinicians are used to relying on evidence-based frameworks and standard clinical policies. In licensing, generic policies create delays when they don’t match: the services you listed the staff roles you actually have the operating model you’re applying under This is why policies and procedures are explicitly required in some provider frameworks (for example, Maryland’s DDA administrative requirements). (law.cornell.edu ) Practical shift: Use templates as a starting point, but make sure policies match your service scope and staffing model exactly. 5) Clinicians try to build the “ideal program” instead of the “licensable first version” Clinicians want to do it right—which often means trying to offer a wide scope: therapy, groups, care coordination, family support, community outreach, crisis response. That’s admirable. It can also slow licensing if your service scope expands faster than your staffing qualifications, supervision structure, and required documentation can support. Practical shift: Start with a clear first version of services you can staff and supervise well. Expand later with a planned pathway. The reassuring truth: clinicians are often great founders once setup is clear Clinicians already have strengths that make licensing easier once you shift the frame: you understand risk and accountability you think in systems (even if you don’t call it that) you value supervision and documentation you care about consistency of service delivery Licensing becomes manageable when you translate clinical thinking into setup decisions.
Where HPI comes in (setup only) This is exactly where clinicians benefit from support: not “paperwork help,” but setup clarity. HPI supports clinician-owners before application submission by helping you: choose the correct licensing / accreditation pathway for your service scope define service scope in plain language with clear boundaries align staffing qualifications and supervision structure to the services align required documentation (policies) so it matches how you will actually operate That reduces the return-revise-resubmit cycle and protects your approval timeline. Bottom line Clinicians struggle with licensing because it’s not about clinical skill. It’s about building a licensable agency structure. Once you lock your service scope, staffing qualifications, supervision structure, and required documentation around the correct pathway, licensing becomes far less mysterious—and much more predictable.
References
- COMAR 10.22.02.10 — Policies and Procedures (example of explicit policy requirements for DDA providers): https://www.law.cornell.edu/regulations/maryland/COMAR-10-22-02-10
- Maryland OHCQ — Residential Service Agencies Overview (example of license category tied to service scope): https://health.maryland.gov/ohcq/Pages/Residential-Service-Agencies.aspx
- Maryland Behavioral Health Regulations Hub (example of program categories and licensing pathways): https://health.maryland.gov/regs/Pages/10-63-01-10-63-06-Behavioral-Health-Regulations-%28.aspx