
Welcome to Health Policy Institute
Medicaid enrollment planning should start during licensing— not after. If you wait until your license is approved to think about Medicaid, you often lose months. Not because you moved “slow,” but because Medicaid enrollment depends on the same setup decisions licensing reviewers look for: service scope, staffing qualifications, supervision structure, and required documentation. Why founders wait (and why it backfires) A common founder mindset is: “First I’ll get licensed. Then I’ll deal with Medicaid.” That sounds logical. But Medicaid enrollment is not a separate project that starts after licensing. It is a connected path. If your licensing setup is unclear—or you end up changing your license later—your Medicaid enrollment timeline usually slips. The simple connection between licensing and Medicaid enrollment Medicaid agencies must verify key facts about providers. One of those is licensing.
Federal rules require State Medicaid agencies to verify that a provider claiming to be licensed is licensed, that the license is not expired, and that there are no current limitations. So Medicaid enrollment depends on your licensing status being clean and easy to verify. If your application submission creates confusion (wrong license type, unclear service scope, staffing not aligned), you don’t just delay licensing—you often delay Medicaid enrollment too. What “planning Medicaid during licensing” actually means (high-level) This is not a step-by-step checklist. It’s decision-making. During licensing, you should already be aligning:.
1) Service scope Medicaid enrollment and billing depend on what services you’re actually authorized to provide. If your service scope is vague or keeps changing, you’re creating enrollment confusion later. 2) Provider type and pathway Medicaid doesn’t enroll “general healthcare businesses.” It enrolls provider types with defined requirements. The Medicaid Provider Enrollment Compendium (MPEC) is CMS guidance that helps states apply federal enrollment and screening rules under 42 CFR Part 455. 3) Staffing qualifications and supervision structure If your services require qualified oversight, Medicaid enrollment reviewers often expect your provider profile and documentation to match that structure. If you “fix staffing later,” you may end up correcting enrollment records later. 4) Required documentation that matches your licensing setup If your documentation package doesn’t match your service scope and staffing model, you risk a licensing delay—and Medicaid enrollment usually can’t move cleanly until licensing is settled. Real-world ways this causes delays
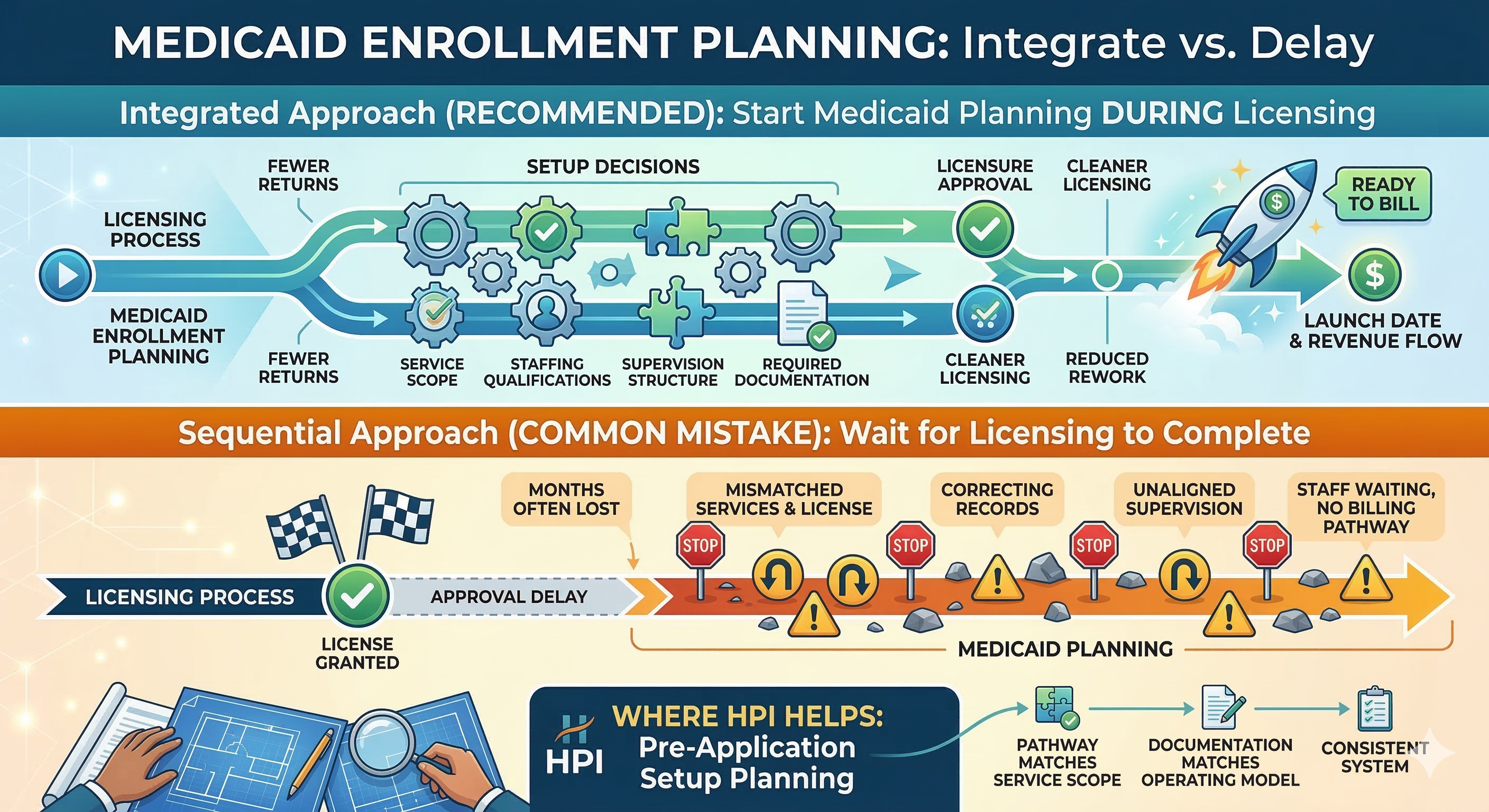
Here’s what it looks like when Medicaid planning starts too late: You get licensed, then realize the license doesn’t match the services you want to bill. Now you’re changing service scope or pursuing a different license, and Medicaid enrollment pauses. Your license is approved, but the service scope is written in a way that doesn’t clearly match the provider type you’re enrolling as. That triggers back-and-forth corrections. Your staffing qualifications don’t line up with the service model you’re enrolling under. You end up revising the supervision structure and resubmitting documentation. You planned your launch date around “license approval,” but Medicaid enrollment adds additional time. You now have staff hired and no billing pathway. The honest takeaway Licensing is the start of your approval timeline. Medicaid enrollment is often what determines your revenue timeline. If you plan Medicaid enrollment during licensing, you reduce the chance of rework—because your licensing setup is designed to support enrollment from day one. If you plan Medicaid enrollment after licensing, you’re more likely to discover mismatches that should have been fixed before the first application submission. Where HPI comes in (pre-application) This is exactly where HPI helps: setup planning before submission.
HPI helps agencies align early so licensing doesn’t create downstream Medicaid problems by ensuring: the license pathway matches the real service scope staffing qualifications and supervision structure support the services required documentation matches the operating model the application submission reads like one consistent system—so approvals don’t stall The goal is simple: fewer returns, cleaner licensing, and a Medicaid enrollment path that’s ready when the license is issued