
Welcome to Health Policy Institute
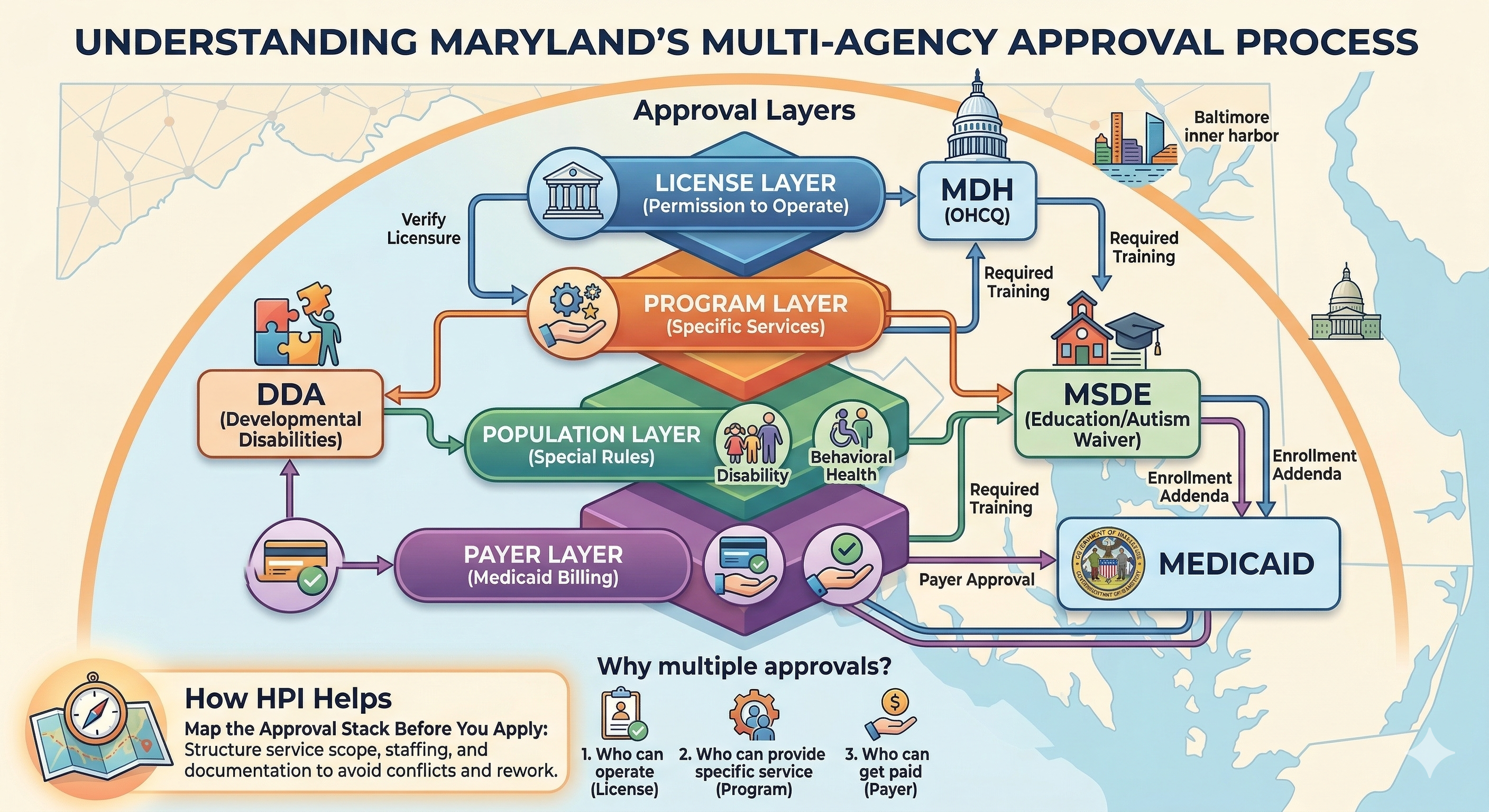
Because one agency usually approves the license, but other agencies may approve the program, the payer, or the population you’re serving. In Maryland, it’s common for one healthcare business to touch more than one system. When that happens, you may need approvals from MDH, DDA, MSDE, and Medicaid—each for a different reason. This isn’t bureaucracy for fun. It’s how the state separates: who can operate, who can provide a specific service, and who can get paid. The simple way to think about it Most multi-approval situations happen because you’re dealing with at least two of these layers: License layer (permission to operate) Program layer (approval to deliver a specific type of service) Payer layer (approval to bill Medicaid) Population layer (special rules for children, disability services, behavioral health, etc.) One agency rarely owns all four layers.
What MDH usually covers (the “permission to operate” layer)MDH is the umbrella department. Within MDH, different offices handle different license categories. Example: OHCQ (Office of Health Care Quality) OHCQ licenses certain provider types, including Residential Service Agencies (RSA). MDH describes an RSA as a business that provides at least one home health care service for compensation, and notes OHCQ is responsible for RSA licensure. Simple example: If you’re starting a home care-style agency under RSA rules, OHCQ is your licensing gate. What DDA covers (the “developmental disability services” layer) DDA oversees the provider framework for developmental disability services in Maryland and points providers to the COMAR regulations that apply. DDA licensing is not the same as “home care licensing.” It’s built around services and supports for people with developmental disabilities—often tied to waiver service models and required provider policies and procedures. Simple example: If your agency is delivering DDA waiver services, you may need DDA approval even if you also have another healthcare license type. What MSDE covers (the “education-linked program” layer) MSDE comes in when the services are tied to school-aged children and education-linked programs—like the Autism Waiver. MSDE publishes Autism Waiver provider information and runs provider trainings/workshops for prospective providers.
Simple example: If you want to provide Autism Waiver services, you may deal with MSDE requirements (like training) because the program is tied to education and child eligibility frameworks—not just healthcare licensing. What Medicaid covers (the “payment approval” layer) Medicaid approval is not the same as licensure. Licensure may let you operate. Medicaid enrollment lets you bill. Maryland Medicaid enrollment for Autism Waiver includes program-specific enrollment addenda, and at least one published addendum states providers must attend the MSDE Autism Waiver initial provider training before enrollment. Separately, federal rules require state Medicaid agencies to verify provider licensure where applicable (meaning licensing status matters for enrollment decisions). Simple example: You can be licensed and still not be able to bill Medicaid until enrollment is completed and verified. Why this creates “more than one approval” in real life Here are common scenarios where agencies need multiple approvals:
Scenario 1: Autism Waiver provider agency MSDE: training/provider readiness activities Medicaid: enrollment to bill for services MDH/DDA: may apply depending on what services you’re delivering and how your agency is structured Scenario 2: DDA provider that also offers nursing-related supports DDA: provider licensing framework and COMAR requirements MDH (OHCQ or other MDH licensing office): may apply depending on the provider type and services Medicaid: enrollment and billing pathway Scenario 3: Behavioral Health agency Behavioral Health is often regulated through MDH’s Behavioral Health Administration (BHA). Maryland explicitly describes “accreditation-based licensing” under COMAR 10.63 for certain behavioral health programs. Then, Medicaid enrollment is a separate step for payment.
What this means for your setup decisions Multi-approval doesn’t mean you should “apply everywhere.” It means you should decide, before applying: What is your service scope (exactly what you will and will not provide)? Which approval is your license to operate versus your program approval versus your payer approval? Do your staffing qualifications and supervision structure match the service scope for each pathway? Does your required documentation match the way each program expects you to operate? When agencies skip these setup decisions, they end up with returned or delayed application submissions—because one approval pathway contradicts another. Where HPI comes in (setup only) This is a classic place agencies lose months: they build one application submission, then discover they actually need a second approval pathway that requires different service scope language, staffing qualifications, supervision structure, and required documentation. HPI helps you map the approval stack before you apply: which regulator approves your license to operate which agency controls the program requirements (DDA, MSDE, BHA) what Medicaid enrollment will require downstream how to structure service scope, staffing, and documentation so the approvals don’t conflict.
Bottom line Some agencies need more than one approval because licensing, program oversight, and Medicaid payment are owned by different agencies. If you understand which approval controls operation, which controls program participation, and which controls payment, you can build a setup that moves faster—and avoid rework.