
Welcome to Health Policy Institute
A founder once told me, “We’re not changing the agency. We’re just adding one service.” Two weeks later, they were rewriting half their setup—because that “one service” quietly changed the rules of the business. That’s the part people miss: expansion isn’t only a marketing decision. It’s a licensing setup decision. Even when your license type stays the same, your agency still has to stay aligned on paper and in structure—or your approval timeline and billing timeline can slow down.
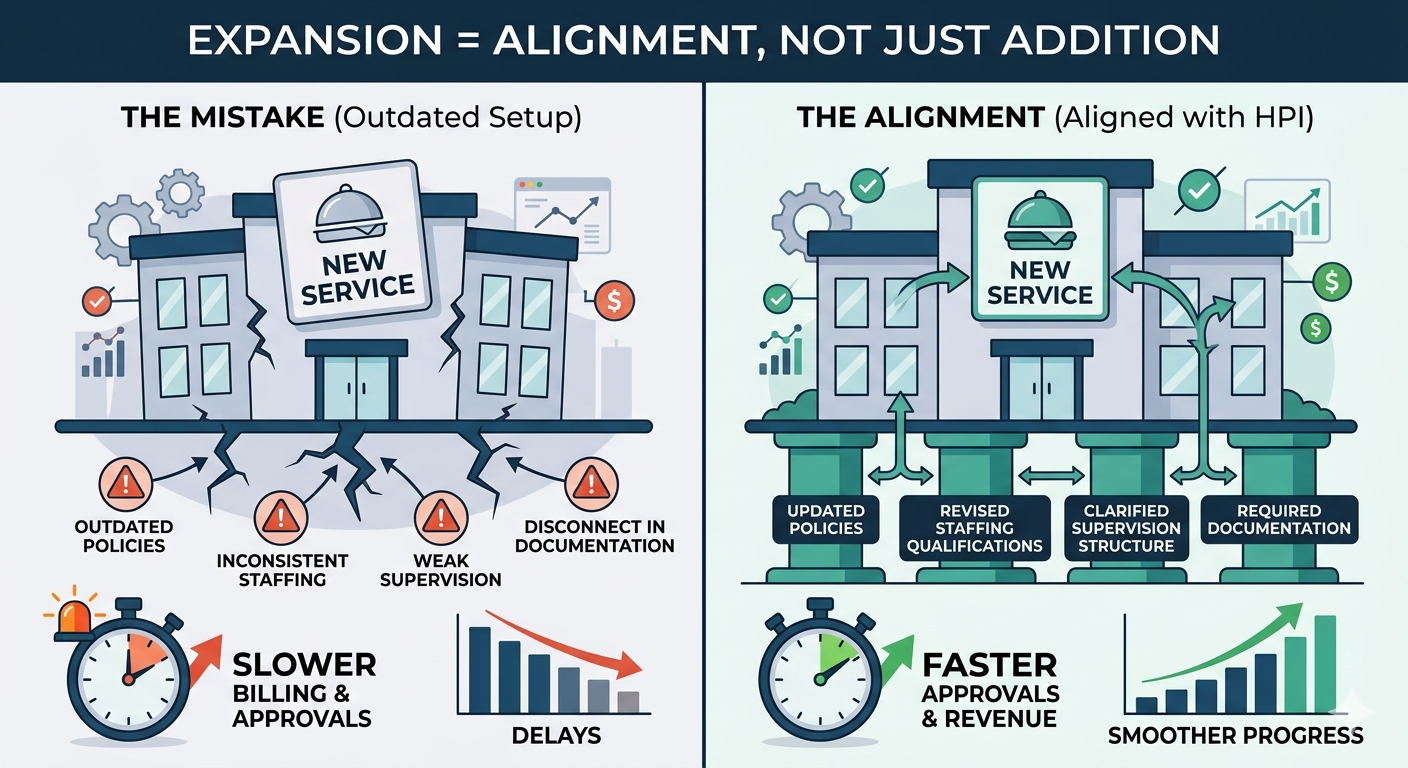
The big idea: adding services changes your setup, not just your menu Licensing reviewers (and payer enrollment teams) don’t evaluate services in isolation. They evaluate whether your agency is set up to deliver the services you say you offer. That means expansions usually require updates in four areas: • Service scope • Staffing qualifications • Supervision structure • Required documentation (especially policies) If any one of those stays stuck in the “old version” of your agency, your package becomes inconsistent. Inconsistency is what creates delays. What usually needs to change during expansion 1) Your service scope (you must redefine the boundaries) When you add services, your service scope needs to be updated to clearly state: • what you now provide • what you still do not provide • what changed from your original model Founder example: You started with non-clinical support services. Now you want to add a service that looks clinical. If you don’t rewrite your service scope clearly, your agency can start sounding like two different business types at once—which is where delays begin. 2) Your staffing model and staffing qualifications (new services often need different credentials) New services often require: • different staff roles • different credentials • different supervision coverage Founder example: You add a service that requires licensed oversight, but your staffing plan is built for support staff only. Even if you plan to hire later, reviewers and payers can only evaluate what your setup shows today.
3) Your supervision structure (expansion often breaks oversight) A supervision structure that worked for one service can fail when you add another. Expansion forces you to clarify: • who supervises the new service • how supervision happens • who is accountable for decisions tied to that service Founder example: “One supervisor oversees everything” worked when your service scope was narrow. After expansion, it may look unrealistic. That triggers questions and slowdowns. 4) Your policies and required documentation (this is where expansion gets stuck most often) Expansion is where generic policies come back to haunt you. When you add services, your policies must be updated so they match: • the expanded service scope • the staff roles you actually use • how supervision will work • what records you will maintain (required documentation) Founder example: You bolt on a policy from a template pack for the new service, but it references roles you don’t have or workflows you don’t follow. Now your documentation contradicts your staffing model, and the agency looks unstable on paper. Some provider frameworks explicitly require agencies to develop and adopt written policies and procedures—so mismatches are not “small.” They’re structural. (Example: DDA provider policy requirements in Maryland.) 5) Your internal “who does what” documents (job descriptions and responsibilities) Expansion almost always requires updating job descriptions because roles change. Common changes include: • new responsibilities for supervisors • new documentation duties • new on-call or coverage expectations • new training expectations tied to the added service If job descriptions don’t match the actual work, reviewers and payers see disconnects.
6) Your licensing and payer story must stay consistent (especially if Medicaid is involved) Even if you do not “change your license,” expanding services can still affect: • whether your services are still inside your approved scope • whether you need an update, modification, or additional approval path • whether your Medicaid enrollment profile needs updates for what you plan to bill Medicaid programs must verify provider licenses where applicable. If your licensing and enrollment story doesn’t match, updates and billing timelines can slow down. A simple expansion check (high-level) Before you add a new service, ask: • Does this service fit our current service scope as approved—or does it change what kind of agency we are? • Do we have the staffing qualifications for this service, or are we hoping to “figure it out later”? • Who supervises this service, and is that supervision structure realistic? • Do our policies clearly support this service without contradictions? If those answers aren’t clear, expansion becomes rework. Where HPI comes in (setup only) Expansion is where agencies accidentally create delays—because they add services without updating the setup. HPI helps you plan expansion the right way by aligning: • service scope to the added service • staffing qualifications and supervision structure to that new scope • required documentation so policies match what you will actually deliver • licensing and Medicaid enrollment planning so expansion doesn’t stall billing The goal is simple: expand without breaking your approvals and timelines
Bottom line When you add new services, you’re not just adding revenue. You’re changing the structure of your agency. Most expansions require updates to: service scope, staffing qualifications, supervision structure, and required documentation—plus job responsibilities and payer enrollment alignment. If you update those on purpose, expansion is smoother. If you don’t, licensing and billing delays show up later—right when you expected growth
References
- DDA Provider Required Policies and Procedures Example (COMAR 10.22.02.10): https://www.law.cornell.edu/regulations/maryland/COMAR-10-22-02-10
- Medicaid Verification of Provider Licenses (42 CFR § 455.412): https://www.ecfr.gov/current/title-42/chapter-IV/subchapter-C/part-455/subpart-E/section-455.412
- Maryland OHCQ RSA Overview (example of licensure tied to service scope): https://health.maryland.gov/ohcq/Pages/Residential-Service-Agencies.aspx