
Welcome to Health Policy Institute
A founder once told me, “We’re licensed now. We’re just going to add one more service.” On paper, it sounded simple. In real life, that “one more service” triggered four new questions: Does our service scope still match our license category? Do we have the right staffing qualifications for the new service? Does our supervision structure support it? Do our policies and required documentation match the new model? That’s the part nobody tells you: adding services isn’t just adding revenue. It’s changing your setup. Sometimes you can add services without changing your license. Sometimes you can’t. Either way, adding services almost always requires setup updates.
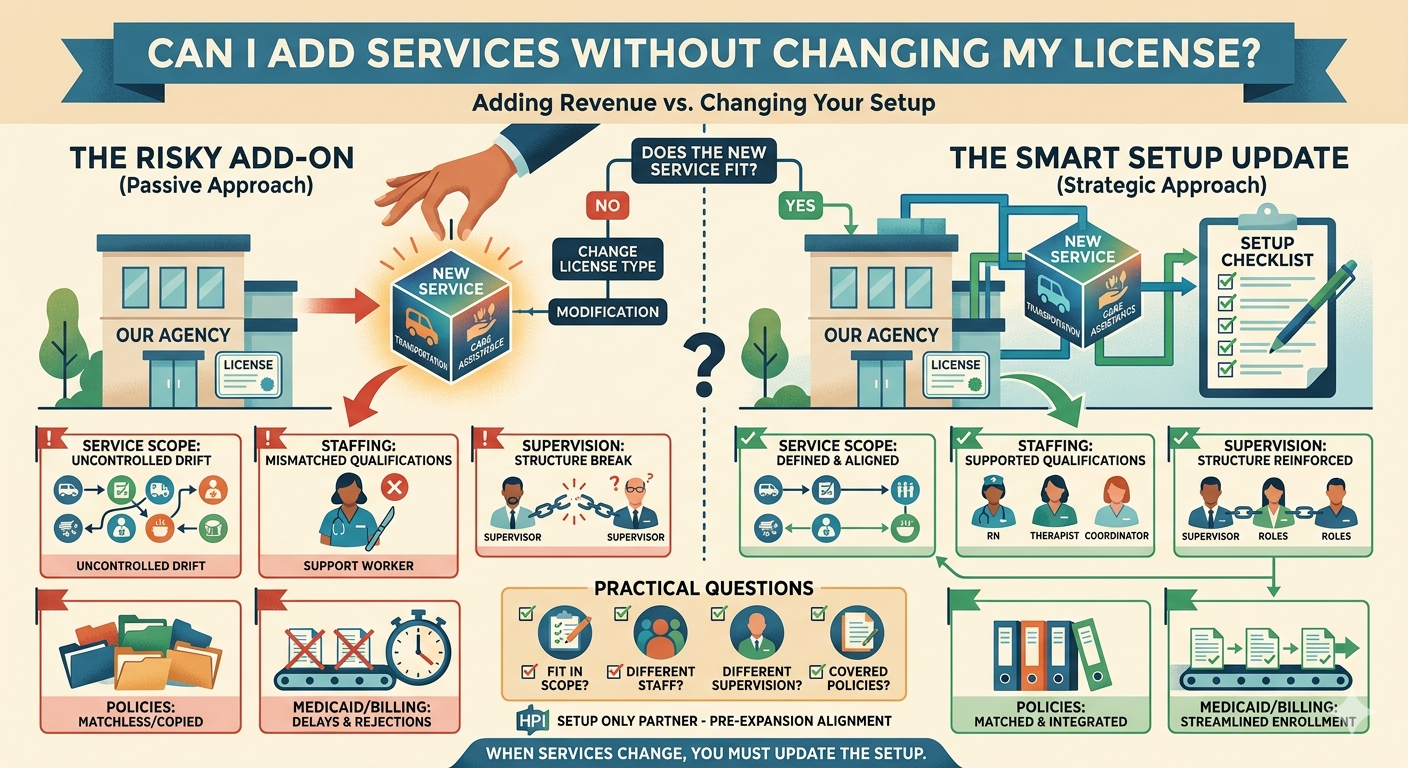
The simple answerYou can add services without changing your license only if the new services fit inside your current service scope and license category. If the new service shifts you into a different service model (for example, from non-clinical support into clinical treatment), you may need: a different license type, or a modification to your existing license approval, or a separate approval pathway The risk is not “getting in trouble.” The risk is operational: your documents stop matching your services, and everything slows down—especially Medicaid enrollment and contracting. Why adding services forces setup updates Licensing reviewers approved you based on a specific story: Here is what you will provide (service scope) Here is who will provide it (staffing qualifications) Here is who supervises it (supervision structure) Here is the required documentation that proves you can operate that model When you add services, you change the story. That means you must update the setup.
5 ways “adding services” creates problems (even when you keep the same license) 1) Your service scope becomes unclear What happens: You start with a clean, narrow scope. Then you add services one by one until the scope reads like “everything.” Founder example: “We started with support services. Now we also do transportation, care coordination, and clinical assessments.” Why it matters: A broader scope often triggers different staffing requirements and documentation expectations. If the scope is unclear, your license and your operations drift apart. 2) Staffing qualifications no longer match the services What happens: Your original staffing model worked for your original services. The new service requires different qualifications. Founder example: Adding a service that needs licensed oversight, but your staffing model is built around support staff. Why it matters: Even if you don’t “change the license,” your staffing qualifications must support the service scope you’re operating under.
3) Your supervision structure breaks What happens: Supervision was simple at first. The new service adds a different kind of oversight requirement, and now accountability is unclear. Founder example: “One supervisor oversees everything,” but now you add a service that requires specialized clinical oversight. Why it matters: If your supervision structure doesn’t match the services, your policies and documentation will also drift. 4) Your policies become mismatched and start to look copied What happens: You bolt on policies for the new service, but they don’t match your existing system. Founder example: Policies mention roles you don’t have, or workflows you don’t actually follow. Why it matters: Policy mismatch is one of the fastest ways to trigger delays when you’re updating licensing, expanding payer enrollment, or entering new contracts. Many provider frameworks explicitly require written policies and procedures, which is why mismatches don’t stay hidden for long. (law.cornell.edu )
5) Medicaid enrollment and billing can get delayed What happens: You add services and plan to bill Medicaid for them, but your enrollment profile, provider type, or documentation doesn’t match the updated service scope. Why it matters: Medicaid agencies must verify provider licenses where applicable. If your licensing and enrollment story is inconsistent, enrollment updates and billing pathways can slow down. (ecfr.gov ) A practical way to decide if a service “fits” your license Before you add a service, ask these high-level questions: Does the new service fit inside our current service scope as approved? Does it require different staffing qualifications than we currently have? Does it require a different supervision structure? Do our policies and required documentation already cover it—or would we be forcing it? If the answer is “we would be forcing it,” treat it as a setup project, not a quick add-on. Where HPI comes in (setup only) Expansion is where good agencies accidentally create delays—because they add services without updating the setup. HPI supports pre-application and pre-expansion setup by helping you:
confirm whether a new service fits your current license scope update service scope language so it stays clear align staffing qualifications and supervision structure align required documentation so it matches the expanded model reduce downstream delays for Medicaid enrollment and contracting Bottom line You may be able to add services without changing your license—but you can’t add services without updating your setup. When services change, you must review and align: service scope, staffing qualifications, supervision structure, and required documentation. That’s how you expand without creating delays you didn’t budget for.